In many cultures, grief is named and sidestepped rather than explored and respected. But, whether in Toni Morrison’s Beloved or The Gathering by Anne Enright, the following books show that grief never truly leaves us; instead, it burrows inside, emerging in big and small ways throughout our lives. In this way, grief has an inherent duality.
It explodes and erodes. It is lament and lacuna, relief and resentment. It is visceral and fugitive. It is shadow and spotlight. Grief can be both burden and revelation, as many of the authors below illustrate. We hope these books help you carry your own grief in a way that respects the uniqueness of that experience, neither forcing pain to the surface nor burying it further inside.
The Mounting Grief of Loss in Womanhood

A poster for the Loss and Grief symposium led by the OMS and National Institutes of Health, 20th century
Grief is a universal experience, but the grieving process does not unfold the same way for everyone. A 2020 study in the Journal of Psychiatric Research reveals (un)surprising differences in how men and women navigate significant loss. It suggests that men tend to experience an acute reaction; they feel immediate devastation after the sudden death of a loved one, but these feelings gradually decrease in the weeks and months that follow.
Many women, however, bear their own grief much differently: their grief may feel less dramatic initially, but it intensifies and lingers over time. Instead of receding as months pass, it only grows. This “mounting grief” is reflected in many of the best books about grief written by women, in which authors process heartbreak that becomes an enduring part of their female characters rather than an isolated experience.
The Burden of Responsibility

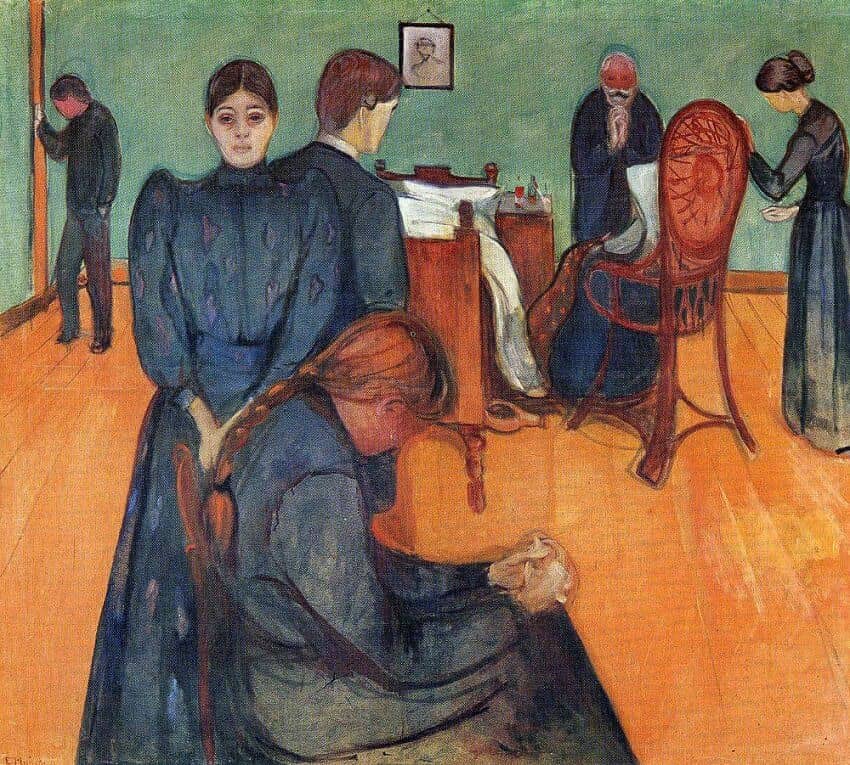
Death and the Child, Edvard Munch, 1889, Oil on canvas, Kunsthalle Bremen, Bremen
Part of this difference comes from the unique challenges women face when mourning. Many women must deal with their grief while caring for children, siblings, or aging parents. Even as they are overcome by sorrow and feel overwhelmed, they may continue to be the emotional center of their families; in this role, they are expected to provide practical advice, offer support, and provide comfort for others while falling apart themselves.
This dual role complicates the healing journey for many women; the mourner must balance her personal anguish with her “duty” of sustaining life for others. Novels written out of women’s own
experiences capture this reality; they echo the fact that dealing with grief is never linear, especially when it is tangled up with caregiving.
How Art Captures Women’s Grief

Lucretia (one of three), oil on canvas, Artemisia Gentileschi, 1627
Despite these lived realities and a growing body of research, cultural portrayals of grief repeatedly flatten or distort women’s experiences. In film and television, women’s mourning is often reduced to wailing at funerals. Their bodies collapse in despair, their hands knot and writhe, mascara-tipped tears fall from their eyes in torrents. Alternatively, men are shown as stoic, resolute, and solemn.
This trope obscures the truth and actually reverses what science has found to be true: women’s grief is rarely a theatrical outpouring of sorrow and men’s grief is not always silent or quickly resolved as such portrayals suggest. Women’s grief is not tidy, either. It can be angry,
messy, violent, and self-destructive; less romantic mascara lines across the cheeks and more empty liquor bottles and stained bedsheets littered on the floor.
*above will be embedded
To illustrate that reality, we turn to art and literature by women. Art created by women (like Tracey Emin’s My Bed or Frida Kahlo’s Henry Ford Hospital) depicts grief and loss as raw and bodied. Literature written by women also resists the clichés outlined above; writers like Carol Shields and Maggie O’Farrell meditate on the complexity, duration, and layered responsibilities of their characters’ grief.
The following books accurately portray how women confront devastating loss, not only of partners, but of children as in Hamnet, of parents as in Everything I Never Told You, and of their own sense of self as in The Stone Diaries. Toni Morrison’s Beloved turns mourning into mythology as she shows how a mother’s grief can be both private and intergenerational. While best known for her deeply personal memoir The Year of Magical Thinking, Joan Didion explores similar territory in fiction like Play It As It Lays, where she writes about dislocation and psychic pain.
Grief as Erosion, Not Explosion

Patience on a monument smiling at Grief, John Roddam Spencer Stanhope (English, 1829 – 1908)
The difference, then, is not about who hurts more, but about the texture and timeline of one’s grief. Men’s mourning may be compared to a storm: violent, visible, then passing. Women’s grief is often better compared to erosion: subtle, relentless, reshaping the landscape of their lives long after others expect them to be “done.”
From Morrison to Enright and from Shields to O’Farrell, literature insists that grief is less something to overcome and more something to integrate. It remakes the self. And it rewrites relationships. The following books are resources for both adults and children, for siblings, parents, and friends, because they show that grief is not only personal but also relational.
In this way, the mounting grief of womanhood is a lesson and a reflection; mourning is not weakness and the refusal to “move on” is not failure. But it shouldn’t be seen solely as a vehicle for personal growth, either. These books might demonstrate the universality of grief, but they also show how deeply individual it is, how fractured it can be, and how nonlinear healing feels.
We encourage you to explore books like Beloved, Runaway, and The Gathering after reading this article. They might not include practical strategies for healing or daily meditations on the complexities of grief, but they do provide context and comfort.
10 Fictional Books About Grief by Women Who Lived Through It
Beloved by Toni Morrison

In this Pulitzer-winning novel by Toni Morrison, Sethe kills her baby daughter rather than see her enslaved, but the child comes back in the form of Beloved after her spirit is forced from their haunted home. Inspired by an account from 1856, the grief in this story is fierce and layered; Sethe (who herself was horrifically abused) mourns her child, but she also mourns her own stolen life and the lives of generations before her.
Over time, Beloved grows larger and larger, fed by Sethe’s guilt-fueled dedication to the young woman. Even as memory of Beloved fades from collective memory in their town, Morrison chronicles how a mother’s sorrow, trauma, and heartbreak lives on in the body and in her own memory. This kind of somatic grief often intensifies (or at the very least, changes shape) with time. It is all-consuming and unending.
The Stone Diaries by Carol Shields

In this novel by Carol Shields, Daisy Goodwill grows up without her mother, who dies in childbirth. Daisy then lives much of her life in obscurity. Long after her mother dies, she endures the death of her husband and her fading sense of self, which debilitates her over time.
Shields traces how loss threads itself through Daisy’s life; her grief is never depicted as a sudden, soul-shattering moment but rather as an undercurrent that slowly shapes who she becomes. This novel makes space for small ways in which grief appears across domestic life.
Here, mourning is not centered on a single devastating event; for her, it is a lifetime of absences.
Runaway by Alice Munro

In this collection by Alice Munro, women live with the grief wrought by abandonment, estrangement, and regret. Children leave home, marriages dissolve, and unrealized possibility dissipates before it can be realized. These stories capture loss not as spectacle but as something that settles slowly into daily life.
Munro shows how women continue moving through ordinary routines while carrying unbearable sorrow with no clear outlet (or outline). Some characters turn away from their feelings, while
others allow themselves to remember and even revel. In either case, grief lingers and shapes the choices Munro’s characters make.
The Gathering by Anne Enright

In Anne Enright’s novel, Veronica Hegarty travels to Dublin after her brother Liam commits suicide. His death forces her to confront the unaddressed fractures and growing silence that have long haunted their family. Here, grief is equally yoked with anger and unease.
Veronica shoulders the weight of holding her family together while privately unraveling. Enright makes visible the hidden burden women often bear in mourning: to soothe others, to tell the story, to carry both memory and responsibility without letting it slip beyond themselves.
Everything I Never Told You by Celeste Ng

Celeste Ng’s novel opens with the sudden death of Lydia Lee, favored daughter of a Chinese American family in 1970s Ohio. The nature of her death is not revealed until much later in the novel. Her mother Marilyn is irreparably undone by the loss, yet her grief is complicated by the expectations she placed on her daughter.
This novel reveals how silence magnifies sorrow and compounds loss. Marilyn aches for the life she wanted for Lydia, while the rest of the family falters under the weight of what has never been said. Ng illustrates how grief can expose every fracture within a household and how mothers, in particular, lie on the sharpest edges of those fractures while trying to desperately to glue them back together.
Hamnet by Maggie O’Farrell

In Hamnet, Maggie O’Farrell reimagines the death of Shakespeare’s young son through the eyes of his mother, Agnes Hathaway who is surprisingly wild and bold. After the shocking death of her son, Agnes feels the boy’s absence in her bones; her mourning is the spine, muscle, and marrow of this book.
O’Farrell writes much from her own brush with death and that closeness to the subject shapes the intensity of her portrayal. She renders the grief of a mother losing a child as both physical and spiritual, something that stretches across time and transforms every relationship it touches.
Critics have described Hamnet as “a luminous portrait of a marriage, a family ravaged by grief.”
The Dark Flood Rises by Margaret Drabble

Margaret Drabble’s novel follows Fran, who is an older woman moving through the cumulative losses that come with age. She attends funerals, witnesses the decline of others she holds dear, and lives with the knowledge that her own mortality is inevitable (and likely near). In Drabble’s novel, grief is an ordinary part of life.
The book does not dwell on widowhood alone but on how women face loss in solitude. Fran resists dependence on others, even as she feels the world narrowing around her. Again, grief is portrayed not as a single shocking event but as a continuum. It grows as we do.
Still, Fran finds the beauty and humor in life, even amid meditations on her own mortality. In The Dark Flood Rises, she opines, “Old age, it’s a fucking disaster!”
The Death of the Heart by Elizabeth Bowen

Elizabeth Bowen’s novel tells the story of sixteen-year-old Portia, who discovers betrayal in her household years after severe loss in her childhood. Instead of a dear relative or romantic partner, she loses her innocence and trust. The grief that follows is quiet but all-consuming.
Bowen wrote out of her own experiences of loss and her prose carries that. Portia’s sorrow is less about sudden death than it is about the collapse of safety she though inherent to being part of a family. Here, grief is tied to betrayal and the unfairness of misplaced trust.
Bowen shows how disillusionment can feel as devastating as bereavement, particularly for a young woman who believed family could be a refuge after losing those closest to her (her father and mother) at an early age.
The Almost Moon by Alice Sebold

In Alice Sebold’s novel, Helen kills her elderly mother after years of tension and care. The act forces her to reckon with a lifetime of estrangement. What follows is grief tangled messily with guilt, anger, and unwanted devotion, emotions many of us feel after complex, conflicting loss.
Being a caregiver is never solely about love; it starts that way, but often devolves into resentment, frustration, and longing for a simpler life with softer boundaries.
Herself a survivor of violence, Sebold writes bluntly without sentimentality. Helen’s mourning is not tender or redemptive; it is complicated and harsh. It exposes the realities of caring for someone out of obligation rather than adoration. The novel explores what it means to grieve a parent one could never fully love.
Many of us are familiar with the anger that comes when a parent, partner, sibling, or friend is “deified” after death. Helen feels anger not just at her mother, but at the way death immediately rewrites her mother’s story. It sands away the uglier, grittier parts that defined their relationship and eroded Helen’s sense of self. Sebold doesn’t soften this but instead shows how grief is tangled with fury when the dead are sanctified.
The Lover by Marguerite Duras

Marguerite Duras’s The Lover is based on her own adolescence in French colonial Vietnam and is not strictly a novel about bereavement, but it explores these themes nonetheless. It illustrates how grief bleeds into many other emotions.
In this book, a young girl enters an affair with an older Chinese man who is quite wealthy. While this affair is central to Duras’ novel, the main character’s deepest pain lies in estrangement from her unstable mother, her brother’s cruelty, and her family’s decline during her absence.
Harshly dislocated from her family, the young narrator feels both estranged from her home and bound to it. Like others on this list, Duras depicts grief that arrives not in a single, deafening blow but in the accumulation of disappointments and separations that percolate over years or even decades. Her novel shows how a young woman grieves for family, for country, and for a
life that could not be lived. The New York Times Book Review described her prose as “powerful, authentic…perfect.”
If You Are Struggling with Grief, Please Consult These Resources

The Widow I (1922–23), woodcut from the Mario de Andrade Collection, Käthe Kollwitz, at the Instituto de Estudos Brasileiros
If you are coping with grief right now, please know that support is available. Grief can feel overwhelming and unending, but you do not have to carry it alone. The following organizations and hotlines can offer you immediate help and ongoing guidance as you navigate the pain of losing a loved one.
● National Alliance for Grieving Children (NAGC)
● National Alliance on Mental Illness (NAMI) Helpline (call 1-800-950-NAMI (6264)) ● 988 Suicide & Crisis Lifeline (U.S.) (dial 988)
● Hospice Foundation of America
Grief may feel isolating, but you are not alone. Finding support, whether through community groups, therapists, or a crisis line, is never a sign of weakness.
A Note from The Somatic Diary
At The Somatic Diary, we have found reading books to be a surprisingly effective way to process trauma and grief; they have become part of our healing process. This may be because literature allows people to witness their own experiences reflected back to them.
The books outlined above navigate and excavate emotions that may otherwise feel overwhelming or unspeakable: shame, anger, hatred, hopelessness, relief, regret… We hope you find some comfort in the many manifestations of grief described by these incredible writers.